|
|
|
| << To Blog Home >> | |
|
What
is |
April 27, 2010 -- 7:05pm EDT See One, Score One for Stents
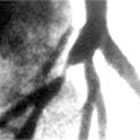
An angiogram doesn't show the cardiologist much about the shape, distribution, or composition of the atherosclerotic plaque: it mainly shows where it is and approximately how long it is. But, seeing inside the artery, the cardiologist is able to discern, for example in the image above, that the plaque is eccentric, all on one side, or perhaps it's ragged or sitting next to calcified deposits. Putting a balloon in and expanding it may push the calcified plaque through the arterial wall, causing a dissection, or the eccentric nature of the lesion may impede the balloon from fully expanding, leaving a less-than-optimal result. Back in the early days of angioplasty, I watched cardiologists as they saw post-balloon angioplasty images from a very early intravascular device: the angioscope -- literally a camera on a catheter. These were among the first cardiologists to ever expand a balloon inside a human coronary artery...and they were shocked. I remember Dr. Richard Myler exclaiming, "My God, it looks like a bomb went off in there!" Indeed, it looked pretty raggedy -- the balloon dilated the artery alright, but the plaque split up during the balloon expansion in a very messy fashion: there was fatty plaque hanging off the sides of the vessel wall and the whole picture showed something definitely not smooth. This was one reason that plain old balloon angioplasty (POBA) had a 30-40% restenosis rate. When stents were invented, cardiologists now had a cage, a scaffold, to push this tissue back against the vessel wall and pin it there. But still, if the plaque were hard, uneven, etc. the stent would not sit quite perfectly, and restensosis or even thrombosis (blood clots) might occur. Enter lesion-specific strategy -- you look at the plaque characteristics and pick the right tool for the job. You have to have an intravascular imaging system to "see one" -- that would be IVUS -- and then, if you saw that the plaque was complex or atypical, you'd need a tool to safely break it up -- and that (in some cases) would be the AngioSculpt® Balloon Catheter. As you can see in the animation below, the nitinol "ribs" on the balloon act as a scoring device. We all know you can't break a piece of glass along a line, but if you score it part-way first with a glass cutter, you can break it perfectly straight. And so, if the IVUS image shows an irregular complex lesion, what's known as a type-C, you might want to pre-treat the plaque, so that when you do expand the stent inside, the plaque expands easily, atraumatically, and smoothly -- seating the stent cozily, right up against the vessel wall.
That's the basic concept of the AngioSculpt balloon, manufactured by AngioScore, Inc. And today Volcano Corporation (Nasdaq: VOLC), makers of IVUS equipment, announced that they are now the distributors for Japan of the AngioSculpt line. It's a perfect fit because it marries distribution of the technology that allows you to "see one" with the technology that allows you to "score one" -- making outcomes for patients better. |
|


 When
the task at hand is performing angioplasty and
placing a stent, the phrase being used more and more is
"lesion-specific strategy". What does this mean? Well, looking
at the angiogram on the left, you can certainly see the lesion, or
blockage...or rather, you can see where the narrowing caused by the
blockage is. You can't actually "see" the lesion itself unless,
of course, you could
get
inside the artery with a camera.
When
the task at hand is performing angioplasty and
placing a stent, the phrase being used more and more is
"lesion-specific strategy". What does this mean? Well, looking
at the angiogram on the left, you can certainly see the lesion, or
blockage...or rather, you can see where the narrowing caused by the
blockage is. You can't actually "see" the lesion itself unless,
of course, you could
get
inside the artery with a camera.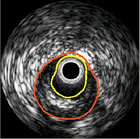 That's
basically what intravascular imaging does: a device is threaded through
the arterial system, along a guide wire (the same wire
that the balloon and/or stent will track) and, using ultrasound
or lasers or near-infrared energy, it will image the inside of the
artery. The most commonly-used system is called IVUS
(IntraVascular UltraSound).
That's
basically what intravascular imaging does: a device is threaded through
the arterial system, along a guide wire (the same wire
that the balloon and/or stent will track) and, using ultrasound
or lasers or near-infrared energy, it will image the inside of the
artery. The most commonly-used system is called IVUS
(IntraVascular UltraSound).