For almost a
half-century, cardiac catheterization, or selective coronary
angiography, has been
the "gold standard"
of imaging tests for determining the nature of coronary artery
disease since
its "accidental" discovery in 1958 by Dr. Mason Sones of the
Cleveland Clinic.
Prior to the
recent development of MultiSlice CT angiography, catheterization
was the only way to directly image the coronary
arteries and
identify areas of narrowing or blockage (technical term: stenosis).
If the cardiologist
determines that an intervention, such as an angioplasty or stent,
can benefit
the
patient, cardiac catheterization is the imaging mode that must be
used for that intervention.
Utilizing
long, flexible, hollow tubes, called catheters, physicians have
been able to
transform the circulatory system of the body into a "highway",
and use it to deliver specialized tools and medicines to diagnose
and treat heart disease non-surgically.
The entrance to the arterial "highway" is
through a needle puncture, usually made in the groin (femoral)
artery. Some physicians have been specially trained to
use the wrist (radial) artery, which is possible in certain
patients and has an advantage of speedier recovery.
Because catheters and devices are actually inserted
inside the body, cardiac catheterization is the only imaging
test that can be called "invasive", unlike the other tests
in this section.
Catheter-based procedures
are performed in a special room in the hospital: the catheterization,
or "cath", lab. The room is
outfitted with high-resolution imaging equipment.
This typically
has been a combination fluoroscopic (X-ray) video and film
system that allowed the cardiologist to
see in
real time what he was doing inside the body. In
recent years, cath labs have become all-digital and now feature
very sophisticated
higher-resolution, finer contrast
and lower X-ray dose technology,
called Flat Panel Detector, or FPD.
Just
before
a coronary angiogram, the patient is given light sedation for
comfort, but remains awake during the procedure in order to respond
to various instructions ("take a deep breath", "hold your
breath", "cough",
etc.)
from the interventional cardiologist who is part operator, part
diagnostician, part photographer.
The first step is a diagnostic
picture of the arteries, called a coronary arteriogram, angiogram
or catheterization. The needle puncture is made, using a local
anesthetic. The physician then threads a catheter through the
entry site and follows the main artery in the body, called
the aorta, up and around into the opening of the left, or right,
coronary artery.
Through this hollow catheter,
the physician injects a small amount of special dye, called
contrast, which, when viewed in motion under X-rays, reveals
any obstructions or plaques located within the coronary vessels.
When the dye is injected, the patient may feel a warm sensation.
Views from several camera angles are recorded. A different
catheter is directed into the heart chamber and dye is
injected into the ventricle, making a ventriculogram, which
shows the movement and efficiency of the heart muscle.
Depending on the number,
severity and location of these obstructions, the physician
may refer the patient for
medical therapy, bypass surgery, or, if appropriate, treat the
patient directly, using catheter-based techniques.
If the likelihood
of coronary blockage was considered high going into the angiogram,
then the patient may have been scheduled for a "cath possible",
short-hand for "catheterization with a possible angioplasty
and stent". In this case, the cardiologist transforms the
diagnostic test on the spot into a therapeutic procedure. Since
the arterial "highway" has already been traversed with
a catheter and guide wire, an angioplasty balloon and stent can
readily be advanced to the blockage and inflated, adding only
about an hour to the session. For more information on this, see Angioplasty
101.
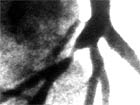
actual
fluoroscopic image of blocked artery artist's
rendering of same
blocked artery
Whether or not an
angioplasty is performed, the puncture site in the femoral artery
must be closed. This can be done with manual compression, which
requires the patient to lie still afterward for many hours while
the puncture site heals. Often small vascular closure devices are
used to seal or close the femoral puncture site. These can be collagen-based
(Angioseal, Vasoseal) where a "plug" of bovine collagen is placed
against the artery to form a seal, or the newest device which is
a nitinol clip (Starclose) and works almost like a grommet punch.
The pros and cons of these various closure methods should be discussed
with the physician beforehand.
As with any invasive procedure, there are some risks to a cardiac
catheterization, although they are rare. The patient may be allergic
to the contrast dye – this should be discussed with the physician
before the catheterization. There is a very slight chance of
heart attack or stroke. The most common complications occur around
the
femoral puncture site. They are less than 3%. Most common is a
hematoma, a bleeding under the skin from a small leak in the closed
artery. Hematomas usually resolve themselves and the bruising appearance
disappears after a few weeks. A larger hematoma, or a pseudo-aneurysm
which is a swelling out of the artery, may require further treatment.
A rare but significant complication is trauma or damage to the
femoral nerve, which runs alongside the femoral artery. If you
experience any complications after your angiogram, contact your
doctor. For more information, read our Discussion Forum topic
on femoral
access site complications.
Whether you should be having a cardiac catheterization, or whether
one of the non-invasive imaging procedures like MultiSlice CT angiography
might be a better screening tool, is a subject each patient needs
to discuss with his or her cardiologist. Recent studies have shown
a cost-risk benefit to the non-invasive tests for certain patient
populations.
Who Does
the Procedure: Cardiac catheterizations
are performed by an interventional cardiologist with his or her
cath lab team of four or more: usually a nurse or two, a cardiovascular
technologist, possibly a physician's assistant or fellow. Be
sure to let the nurse or physician know if you experience anything
out of the ordinary.
Patient
Preparation:Don't eat or drink
for six to eight hours before the angiogram. Make sure your doctor
or nurse practictioner knows ahead of time all the medications
you are currently taking in case one needs to be stopped. Also
tell your doctor if you are diabetic or have allergies of any
sort. Once admitted, you'll be given some standard checks and
the area around the puncture site will be shaved. Every hospital
has their own protocol. It's very helpful if you have a family
member or friend with you. A simple angiogram is usually done
as an outpatient procedure and you will go home the same day.
send comments & suggestions
to "info at angioplasty dot org"
Read our Privacy statement.
Angioplasty.Org is an editorially independent informational health
site
which has received unrestricted educational grants from Medtronic plc,
TCROSS NEWS, Toshiba
America
Medical Systems, Volcano
Corporation, Terumo
Medical Corporation
Cardium Therapeutics, Inc. and Lenox Hill Heart and Vascular Institute of NY