|
New Intravascular Ultrasound
(IVUS) Study of Underexpanded Stents, Thrombosis and Restenosis
|
 |
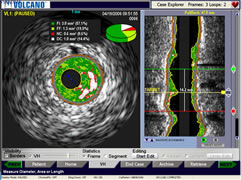
A 2D (left)
and 3D reconstruction (right) of a
coronary
artery using intravascular
ultrasound
(IVUS) --
the
colored areas represents plaque |
|
May 19,
2009 --
A study, published in the current issue of JACC Interventions,
details 120 drug-eluting stent cases as viewed by intravascular
ultrasound (IVUS) in order to examine characteristics that may
lead to in-stent restenosis (ISR) or stent thrombosis.
Underexpansion of stents, both drug-eluting and bare metal,
has been long identified as a significant predictor of adverse
clinical events. Prominently discussed by Dr. Antonio Colombo
in the early days of stenting, inadequate expansion of the
stent struts is known to increase these problems. |
This latest examination studied whether there was
a difference in the type of underexpansion that caused thrombosis
(blood clotting) versus in-stent restenosis (the growth of excess
tissue inside the stent) in drug-eluting stents (DES). Dr. Akiko
Maehara
and a team from the Cardiovascular Research Foundation and Columbia
University
Medical
Center in New
York looked at 20 definite DES thrombosis patients, which represented
all definite thromboses from 1,407 consecutive DES patients
who underwent intravascular ultrasound imaging. These were
compared to 50 risk-factor-balanced ISR patients with no evidence
of stent
thrombosis
and 50 risk-factor-balanced "no-event" patients
with neither thrombosis nor ISR.
Using IVUS allows the cardiologist to see
not only the amount of blockage, as in a 2D angiogram, but the spatial
and volumetric relationship of the blockage to the actual arterial
wall in three dimensions. An issue with inadequate
stent expansion is that, using angiography alone,
the
operator may
not be sure that the stent struts are pressed up against the interior
surface of the coronary artery. Additionally, by using a 3D
real-time reconstruction of an IVUS "pull-back" (the right
image above), the interventionalist can see
immediately after stent implantation any eccentricities
of the
arterial segment and can ensure that full expansion has occurred.
If
the stent
is
not
adequately expanded, the placement can be "touched-up" with
a high-pressure balloon expansion in all or part of the stent. Incomplete
expansion allows a space to exist between the stent struts and arterial
wall, a space where thrombus can form and can also promote
unwanted tissue growth which then blocks the stent.
85% of the thrombosis studied in this report
occurred within 30 days of the stent procedure, pointing up the fact
that inadequate placement, not the drug or polymer or other characteristics
of the drug-eluting coating, was the prime predictor. The study concluded,
however, that there is a difference between underexpanded stents
that thrombose versus
underexpanded
stents that restenose: the underexpansion in DES that thrombose
is more severe, more diffuse, and more often proximal in location.
The researchers found that in cases of thrombosis, the proximal parts
of many of the stents were inadequately expanded,
possibly because stents are usually sized more for the center
and distal ends of blockages where there is more disease.
The past few years have seen an increase in the
the use of IVUS during procedures. Reports, such as this one, may
give further momentum to the ability of this imaging modality to
positively impact patient outcomes. In an accompanying editorial,
Drs. Karan S. Bhalla and H. Vernon "Skip" Anderson
of the University of Texas Health Science Center, Houston, summarize
one of the main take-away messages of this study:
| "Inadequate
deployment is responsible for at least some of the adverse
clinical events of thrombosis and restenosis
that continue to haunt us. Adequate stent expansion throughout
the entire stent length must be the goal. All of this might
mean a greater use of IVUS to check for optimal stent expansion.
The devotees of IVUS will continue to champion this approach,
and for those who prefer IVUS but have been constrained by
outside forces, the justification for IVUS has never been
greater.... Only by taking the necessary time and paying
close attention to detail will we be able to reduce the contribution
that
inadequate DES expansion makes to these insidious phenomena." |
|

H. Vernon "Skip" Anderson,
MD, FACC, FSCAI |
Reported by Burt Cohen, May 19, 2009
|

