Transradial Cardiac Catheterizations
Using
Optitorque™ Catheters
Jared S. Corriel, M.D.
Cardiology Fellow, Beth
Israel Medical Center
Tak W. Kwan, M.D., F.A.C.C., F.A.C.P.
Senior Associate
Director of the Cardiac Catheterization Laboratory and Interventional
Cardiology,
Beth Israel Medical Center, Associate Clinical Professor
of Medicine, Albert Einstein College of Medicine
|
Background
Transradial access for coronary catheterizations
has become increasingly popular worldwide. Compared to the traditional
femoral access technique, transradial access results in less major
and minor access site bleeding
(1). Early ambulation, another benefit of the transradial approach,
results in a significant reduction in patient morbidity. Further,
aortoiliac disease, occasionally found in those presenting for coronary
catheterization, is not an issue when using transradial access (2,3).
The
transradial approach is used in only 7% of coronary angiograms in
the United States compared with approximately 50% in Asia, and
40% in Europe. Less widespread adoption in the US may be due to the
inability to introduce larger equipment and intra-aortic balloon
pumps through the radial artery, arterial spasm, and the need for
additional training with the technique. Radial artery spasm complicates
transradial catheterizations in 2-6% of cases (4,5). Difficulty
accessing the relatively narrow radial artery and increased need
for catheter manipulation for coronary engagement by less-experienced
operators can also result in longer procedure times.
Optitorque Catheter Advantages
Catheters commonly used during cardiac catheterizations are designed for ease
of coronary engagement from a transfemoral approach. While these catheters
are routinely used for transradial angiography, coronary engagement usually
requires more technical skill when used from the radial artery. Optitorque
catheter provides a solution to this problem. The design of these catheters,
which include the “Tiger Catheter” and “Jacky Catheter” are
such that a full coronary angiogram and left ventriculogram can be performed
with a single catheter. Reduced catheter exchanges and movements result in
less radial artery spasm, radiation exposure and procedure time. Small but
important design differences between the catheters should be noted. The “Jacky” has
a less acute terminal curve, which has a tendency to sit more coaxial with
the left main coronary artery and engage the right coronary artery with fewer
movements than the “Tiger Catheter.”
Disadvantages
When performing
a left ventriculogram, a hand injection via the Optitorque
may be inadequate; exchange
for a pigtail catheter with a power injector may be necessary.
In addition, the Optitorque catheter tip frequently points
directly towards the anterior wall of the left ventricle causing
ventricular
ectopy.
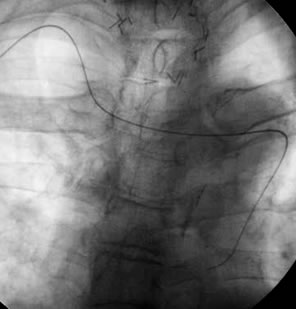
Care must be taken to avoid contrast
staining during a hand injection. When engaging the right
coronary artery,
the Tiger catheter often selectively engages the conus branch
of
the right coronary artery (Figure 1).
As with all equipment,
there is a learning curve. |
|
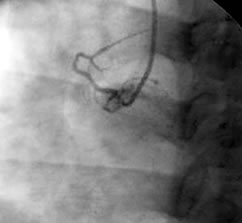
Figure
1. Selective conus branch of the
right
coronary artery by the
Optitorque catheter. |
Technique
Our systematic approach to transradial cardiac
catheterizations using an Optitorque catheter begins with a modified
Allens test
to assess the competency of the ulnar artery in supplying the radial
artery territory. A waveform on the pulse oximetry monitor while
occluding the radial artery indicates suitable dual blood supply
of the hand (6). A 5 French Glidesheath is inserted transradially
using the counter-puncture technique. A combination of Verapamil
2.5mg, Nitroglycerin 100 mcg, and 2500 units of Heparin is then flushed
into the sideport of the sheath (4).
With sheath insertion, a 260
cm wire is advanced via the Optitorque catheter through the radial
artery down the ascending aorta to the aortic valve. The catheter
is advanced over the wire to the valve, and the wire is passed into
the left ventricle. The catheter is then moved into the mid-cavity
of the ventricle and turned so the tip is facing the anterior ventricular
wall in an RAO projection. A small hand test injection insures
avoidance of contrast staining of the ventricle (Figure 2A). A left
ventriculogram is then performed by hand injection (Figure 2B).
|
|
 |
Figure
2 (A). A small hand test injection of left ventricle by
Optitorque (Jacky) catheter.
(B). A left ventriculogram
by hand injection of the Optitorque (Jacky) catheter. |
The catheter is then pulled back slowly into the
aorta and torqued slightly so that the tip is pointing up and to
the left. The Optitorque catheter is advanced downward until it approaches
the left main artery. The catheter is pulled back slightly with gentle
clockwise and counter-clockwise rotations until the left main artery
is engaged (Figure 3A and 3B).

|
|
 |
Figure
3 (A). Optitorque (Jacky) engaging the left coronary artery.
(B). Optitorque (Tiger) engaging the left coronary artery. |
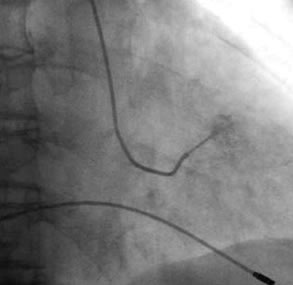
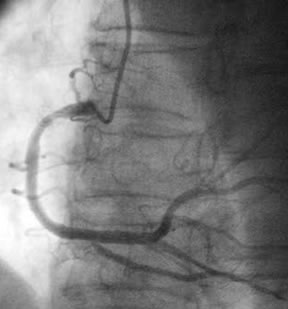
Once
angiography of the left coronary system is complete, the
catheter is disengaged by pulling back slightly. With a clockwise
torque, the catheter is advanced simultaneously until it
points down toward the right cusp. The catheter is advanced
until the right coronary artery is engaged (Figure 4).
Following
angiography of the right coronary artery, the catheter
is disengaged by torquing out of the artery, and the catheter
is removed over the wire.
The sheath is then removed and
local pressure applied by the TR Band special radial
closure bracelet. . |
|
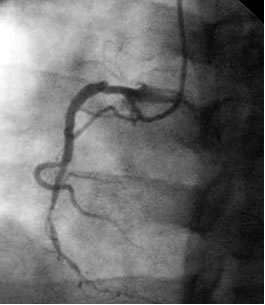
Figure 4.
Selective right coronary artery angiogram by the Optitorque
(Jacky) catheter. |
Personal Experience
Over 400 transradial cardiac
catheterizations using Optitorque catheters have been performed at
our institution, Beth Israel Medical Center, in New York City with
a >95% success rate. In our experience at this academic institution
with an active cardiology/interventional cardiology fellowship program,
approximately 10 procedures are required for an operator to gain
comfort and proficiency with the transradial catheterization using
the Optitorque catheter. The procedure time for a simple diagnostic
left heart catheterization from guidewire insertion to the completion
of the study is typically less than 5 minutes.
In patients with tortuosity
of the subclavian artery or aortic arch, Optitorque catheters generally
engage the right coronary artery without difficulties (Figure 5A
and 5B). In extreme cases, we upgrade to a larger Optitorque (Tiger
4.5 or Sarah) catheter.
|
|
 |
Figure
5 (A). Tortuosity of the aorta. (B). Successful
engagement of the right coronary artery by the
Optitorque
(Tiger)
catheter despite tortuosity of the aorta. |
Conclusions
Transradial cardiac catheterizations
are an increasingly popular method for coronary angiography. In experienced
hands, coronary angiography using an Optitorque catheter with the
technique described significantly reduces procedure cost and time,
complications, and patient discomfort. Thus, the Optitorque is our
first choice for transradial catheterization.
References
- Kiemeneij
F, Laarman GJ, Odekerken D, et al. A randomized comparison
of percutaneous transluminal coronary angioplasty by the radial,
brachial and femoral
approaches: the access study. J Am Coll Cardiol. 1997
May;29(6)1269-75
- Hildick-Smith DJR, Lowe MD, Walsh JT, et al. Coronary
angiography from the radial artery-experience, complications
and limitations.
Int J Cardiol. 1998 May 15;64(3):231-9
- Agostoni P, Biondi-Zoccai
GG, de Benedictis ML, et al. Radial versus femoral
approach for percutaneous coronary diagnostic and
interventional procedures; Systemic
overview
and meta-analysis of randomized trials. J Am Coll
Cardiol. 2004 Jul 21;44(2):349-56
- Coppola J, Patel T, Kwan T, et al.
Nitroglycerin, nitroprusside, or both, in preventing radial
artery spasm during transradial artery catheterization.
J. Invasive Cardiol. 2006 Apr;18(4):155-8
- Saito S, Tanaka S, Hiroe Y, et al.
Usefulness of hydrophilic coating
on arterial sheath introducer in transradial
coronary intervention. Catheter Cardiovasc
Interv. 2002
Jul;56(3):328-32
- Barbeau GR,
Arsenault F, Dugas L, et al. Evaluation of
the ulnopalmar arterial arches with pulse oximetry
and plethysmography.
Am Heart J. 2004
Mar;147(3):489-93
Published Online: September 15, 2008 -- Angioplasty.Org
|