|
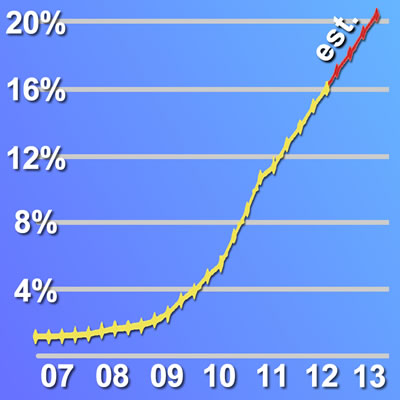
This important retrospective study of data from the CathPCI Registry confirms what several interventional cardiologists told Angioplasty.Org last month ("Transradial Approach Surging in the U.S."). Stents are now being placed via the wrist 15-20% of the time in the United States. When Angioplasty.Org created its Radial Access Center in 2007, only 1.2% of PCIs were done using the radial artery. As of September 2012, that figure had increased to 16.1%. Extrapolating that trajectory in the graph above, Angioplasty.Org predicts that 20% of all stent procedures in the U.S. will be performed using the transradial approach by the end of 2013. Given this extremely rapid growth of wrist angioplasty, some experts like Dr. Sanjit Jolly of McMaster University in Canada, principal investigator for the RIVAL study, predict 50% adoption in three to five years. These data represent a sea-change for the specialty of interventional cardiology in the United States.
The United States has lagged behind other countries in adoption of new technologies, like radial access. The study's lead author, Dr. Dmitriy N. Feldman, assistant professor of medicine at Weill Cornell Medical College, New York Presbyterian Hospital Department of Medicine, Greenberg Division of Cardiology, stated, "Traditionally, femoral access has been taught and used in the United States for PCI, whereas the radial approach is frequently used in Europe." Indeed, the radial approach is used 50% of the time in many countries around the world today. Brachial, Femoral, Radial In 1989, Dr. Lucien Campeau in Montreal, published his seminal work, describing his experience of 100 diagnostic coronary angiographies done via the wrist/radial approach. Three years later, Dr. Ferdinand Kiemeneij's group in Amsterdam first performed interventions using the radial artery. Slowly the wrist technique spread on the Continent, and also to India and Japan. But not to the United States. Until now. Data Supports Safety, Cost and Potential Superiority of Radial Approach These physicians, like Drs. John Coppola and Tift Mann, returned to the U.S. and began training their colleagues and Fellows in the radial technique. Others studied in Canada and brought their training back. Radialists, as they are called, appeared in clusters, or "islands" as Dr. Tejas Patel describes them. In fact the Circulation study shows that there are significant regional disparities in the practice of radial procedures: wrist PCI is far more prevalent in the Northeastern U.S. It was also clear that there are many hospital centers (approximately 13%) that do no radial cases at all. However, all that is necessary to significantly change that is for a radial cardiologist to enter a practice. Most radialists perform 80-90% of their cases via the wrist, using a "radial first" strategy. And typically, when the staff and colleagues see the results, and see patients standing up and walking immediately after their procedures, adoption spreads. One interesting fact pointed out in the study was that almost half of all femoral procedures make use of vascular closure devices, such as Angio-Seal, StarClose, Perclose, etc. These devices have the benefit of quicker time to hemostasis and earlier ambulation of the patient, but they add a cost of $200-300 per procedure and unfortunately have their own subset of complications. One of the interesting and attractive features of the transradial approach is that there is little or no additional cost or special equipment involved. Safer for High-Risk Patients, But Used Less Training, Equipment and Patient Education About The Radial Access Center on Angioplasty.Org This June, Angioplasty.Org joins with Medtronic to promote "Transradial Awareness Month." During this month Angioplasty.Org will be posting interviews with leading practitioners of the radial technique, and feature special articles detailing the advantages of the transradial techniques, and opportunities for physicians and cath lab staff to learn the technique, through a listing of upcoming training courses in the transradial approach. For patients there is also a "Hospital Locator" that lists U.S. centers practicing radial angiography. As Dr. Howard Cohen of Temple University Hospital in Pennsylvania says of the wrist technique, "Patients really prefer it. 95% of people who've had it both ways would say 'I'm coming back to you, Dr. Cohen because I like this transradial a lot better than the other way!' Reported by Burt Cohen, June 10, 2013 |