
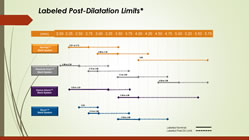
click for hi-res PDF of chart
For the interventionalist, proper sizing of coronary stents is critical. While imaging via angiography has been the standard for years, newer intravascular imaging technologies, such as IVUS and OCT, are becoming more widely used, as evidence accrues that these modalities make a difference in outcomes. For example, IVUS (Intravascular Ultrasound) not only allows the measurement of the exact open diameter of the vessel, as seen on angiography, but it shows the “invisible to angiography” layer of plaque. plaque that will be compressed, so that a more accurate post-PCI diameter can be determined. Under-expanded stents have been associated with increased stent thrombosis and restenosis. Continue reading

 On September 22-23, 2016, the 5th Advanced International Masterclass on the Transradial Approach will be held in Budapest, Hungary. And this year, AimRADIAL will be preceded on September 21 by a one-day comprehensive workshop covering all aspects of Fractional Flow Reserve (FFR) from the basic principles and set-up in the cath lab, to the differences between FFR, iFR, and CFR, a comprehensive review of the clinical study data so far, and finally a look at future modalities, like FFR-CT (although the title of that talk by Dr.
On September 22-23, 2016, the 5th Advanced International Masterclass on the Transradial Approach will be held in Budapest, Hungary. And this year, AimRADIAL will be preceded on September 21 by a one-day comprehensive workshop covering all aspects of Fractional Flow Reserve (FFR) from the basic principles and set-up in the cath lab, to the differences between FFR, iFR, and CFR, a comprehensive review of the clinical study data so far, and finally a look at future modalities, like FFR-CT (although the title of that talk by Dr.  This past week saw publication of an update to the 2007 COURAGE trial which compared optimal medical therapy (OMT) to stenting (PCI) as the initial management strategy for stable coronary artery disease. (Please note the phrase “initial management strategy.” This will not be the last time you see it in this post.)
This past week saw publication of an update to the 2007 COURAGE trial which compared optimal medical therapy (OMT) to stenting (PCI) as the initial management strategy for stable coronary artery disease. (Please note the phrase “initial management strategy.” This will not be the last time you see it in this post.)
 Rumors and theories about an acquisition of Volcano Corporation (NASDAQ: VOLC) had been circulating for quite some time: months, years even. The company seemed an obvious choice: it has an advanced intravascular ultrasound (IVUS) technology that leads the market, with Boston Scientific coming in second; it has a fractional flow reserve (FFR) wire that splits the market with St. Jude Medical; and recently
Rumors and theories about an acquisition of Volcano Corporation (NASDAQ: VOLC) had been circulating for quite some time: months, years even. The company seemed an obvious choice: it has an advanced intravascular ultrasound (IVUS) technology that leads the market, with Boston Scientific coming in second; it has a fractional flow reserve (FFR) wire that splits the market with St. Jude Medical; and recently 


