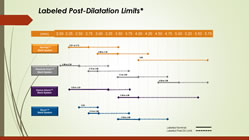
click for hi-res PDF of chart
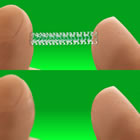
For the interventionalist, proper sizing of coronary stents is critical. While imaging via angiography has been the standard for years, newer intravascular imaging technologies, such as IVUS and OCT, are becoming more widely used, as evidence accrues that these modalities make a difference in outcomes. For example, IVUS (Intravascular Ultrasound) not only allows the measurement of the exact open diameter of the vessel, as seen on angiography, but it shows the “invisible to angiography” layer of plaque. plaque that will be compressed, so that a more accurate post-PCI diameter can be determined. Under-expanded stents have been associated with increased stent thrombosis and restenosis. Continue reading

 Last night news began circulating on Twitter that Abbott’s Absorb BVS (Bioresorbable Vascular Scaffold) was being withdrawn from the European market. This information was prompted by several physicians posting on Twitter a March 31 “Urgent Field Safety Notice/Physician Advisory” letter from Abbott addressed to “Valued Abbott Vascular Customer.”
Last night news began circulating on Twitter that Abbott’s Absorb BVS (Bioresorbable Vascular Scaffold) was being withdrawn from the European market. This information was prompted by several physicians posting on Twitter a March 31 “Urgent Field Safety Notice/Physician Advisory” letter from Abbott addressed to “Valued Abbott Vascular Customer.”
 At this week’s annual European Society of Cardiology Congress in Rome, an important randomized clinical trial on stents was presented by Professor Kaare H. Bønaa, MD, PhD of the Clinic for Heart Disease, St. Olav’s University Hospital in Trondheim, Norway. Called NORSTENT, short for the “Norwegian Coronary Stent Trial,” this was the largest stent trial ever conducted, with 9,013 patients followed for six years. That’s serious!
At this week’s annual European Society of Cardiology Congress in Rome, an important randomized clinical trial on stents was presented by Professor Kaare H. Bønaa, MD, PhD of the Clinic for Heart Disease, St. Olav’s University Hospital in Trondheim, Norway. Called NORSTENT, short for the “Norwegian Coronary Stent Trial,” this was the largest stent trial ever conducted, with 9,013 patients followed for six years. That’s serious!  This past week saw publication of an update to the 2007 COURAGE trial which compared optimal medical therapy (OMT) to stenting (PCI) as the initial management strategy for stable coronary artery disease. (Please note the phrase “initial management strategy.” This will not be the last time you see it in this post.)
This past week saw publication of an update to the 2007 COURAGE trial which compared optimal medical therapy (OMT) to stenting (PCI) as the initial management strategy for stable coronary artery disease. (Please note the phrase “initial management strategy.” This will not be the last time you see it in this post.)